Online Course
NRSG 780 - Health Promotion and Population Health
Module 2: Determinants of Health
Modifiable Lifestyle Risk Factors: High Blood Pressure
Another modifiable lifestyle risk factor for the leading causes of death is high blood pressure. This subtopic will focus on the effects, risks and trends associated with high blood pressure.
Until the early 1960s blood pressure was thought to rise with age. The Framingham Heart Study first identified hypertension as a risk factor in the development of coronary heart disease in 1961(1).
- Kannel, W., Dawber, T.R., Kagan, A., Revotskie, N., & Stokes, J. (1961). Factors of risk in the development of coronary heart disease—Six year follow-up experience. Annals of Internal Medicine, 55(1), 33-50.
Research conducted by the Veterans Administration Cooperative Study Group on Antihypertensive Agents beginning in 1963 also challenged this assumption and showed that treatment dramatically reduced the risk of a morbid event from over a five year period and that treatment also reduced the risk of heart failure and stroke. In part two of the study, the differences between the participants in the treated and control (taking placebos) groups were so dramatic that the trial was terminated early. (2, 3)
- VA Cooperative Study Group. (1967). Effects of treatment on morbidity in hypertension, Journal of American Medical Association, 202(11), 1028-1034.
- VA Cooperative Study Group, (1970). Effects of treatment on morbidity in hypertension II. Results in patients with diastolic blood pressure averaging 90 through114 mm Hg, Journal of the American Medical Association, 213(7), 1143-1152.
The five-year findings of the Hypertension Detection and Follow-up Program (HDFP) Cooperative Group of nearly 11,000 community-based participants from 30-69 showed that a program of stepped care as compared to referred care achieved better control of hypertension and significant reductions in mortality. The study concluded that systematic effective management of hypertension has a great potential for reducing mortality for the significant number of people with high blood pressure in the population, including those with mild hypertension (4).
- HDFP Cooperative Study Group. (1979). Five-year findings of the hypertension detection and follow-up program I. Reduction of mortality of persons with high blood pressure, including mild hypertension, Journal of the American Medical Association, 242(23), 2562-2577.
Risks of High Blood Pressure
High blood pressure significantly increases the risk of:
- Stroke
- Coronary heart disease
- Congestive heart failure
- Aneurysm
- Kidney failure
- Vision changes
Trends in High Blood Pressure
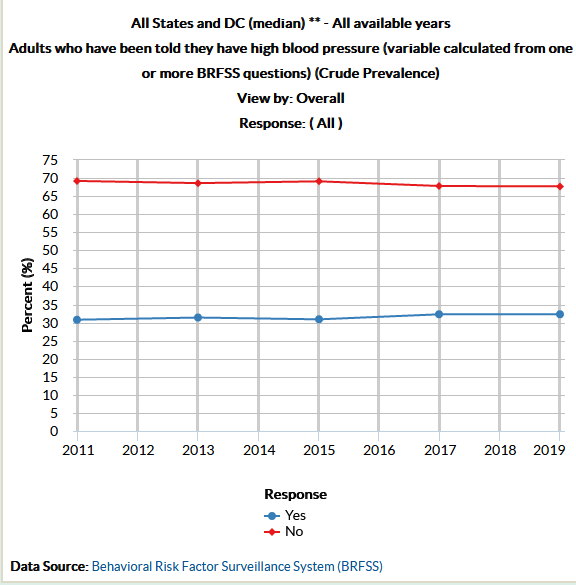
In the U.S. trends show that there has been a slight increase in high blood pressure during the past decade with roughly a third of the population indicating that they have blood pressure in excess of 140/90.
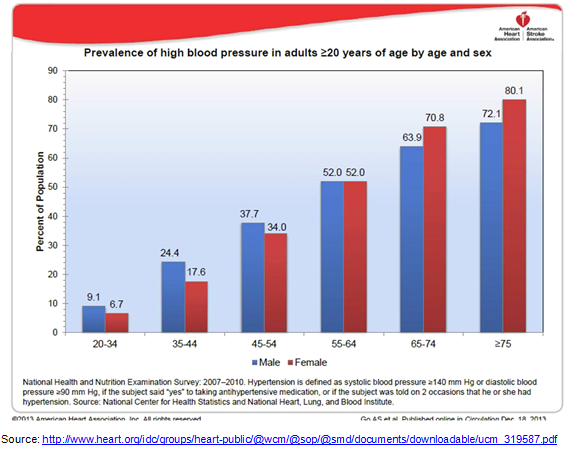
In the U.S. blood pressure increases with age. Blood pressure is higher in men at younger ages. It shifts to being higher in women 45 and over, when menopause occurs, and stays higher than in men for their lifespan.
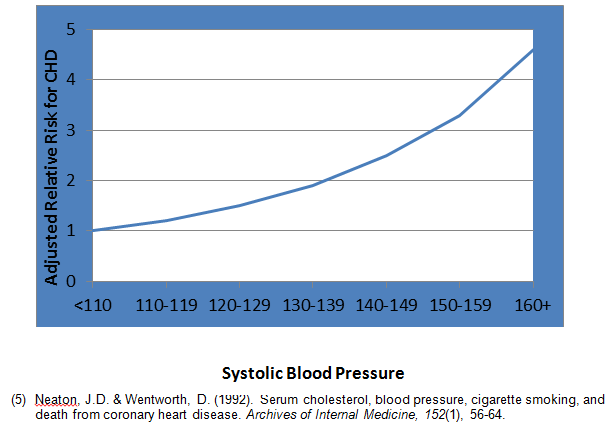
As blood pressure increases, the risk of developing blood pressure related diseases increases. The relative risk of developing CHD is twice as high when systolic blood pressure is in the 130-139 range as compared to below 110, and 4.5 times as great when systolic blood pressure exceeds 160 (5).
Relative Risk of Developing CHD vs. Systolic Blood Pressure
Data from the NHANES surveys show that trends in adults in blood pressure awareness, treatment and control are far from ideal. This is particularly noteworthy given the risk of preventable disease, the toll of diseases such as stroke, and the well-documented effectiveness of anti-hypertensive treatment.
The last two surveys defined high blood pressure as >130/80 as compared to the previous surveys that used 140/90 as the standard. Of the population that has high blood pressure59% are aware, and only 21% are under control. This downward trend is alarming as control levels had been improving slightly for over 30 years until 2017.

SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2011–2012, 2017-2018. Retrieved from http://www.cdc.gov/nchs/data/databriefs/db133.htm, https://www.cdc.gov/nchs/products/databriefs/db364.htm, and https://www.cdc.gov/nchs/products/databriefs/db511.htm
When we consider the unacceptably low level of control and the fact that by the time Americans reach age 74, nearly 75% of the adult population has high blood pressure, it is clear that uncontrolled hypertension plays a significant role in the health status of the US population as a whole.
Question:
Dr. Carolyn Clancy, former Director of the Agency for Healthcare Quality and Research (AHRQ), gave The Dean’s Distinguished Virginia Lee Franklin Lecture at the School of Nursing in 2011. She identified our inability to control high blood pressure, given our arsenal of treatment options, as one of the greatest failures of our health care system. This dilemma has only grown worse in the past decade. Can you identify possible interventions at the community, provider and policy level that may help to improve the level of control?
This website is maintained by the University of Maryland School of Nursing (UMSON) Office of Learning Technologies. The UMSON logo and all other contents of this website are the sole property of UMSON and may not be used for any purpose without prior written consent. Links to other websites do not constitute or imply an endorsement of those sites, their content, or their products and services. Please send comments, corrections, and link improvements to nrsonline@umaryland.edu.