Online Course
NDNP 819: Advanced Health Assessment Across the Lifespan
Module 3: Cardiovascular, Respiratory, and Abdomen
Cardiovascular System
History Components
With all history questions you are trying to assess 2 angles: what is going on now and what they are at risk for which translates across practice areas. A thorough assessment of history will translate to better patient outcomes whether inpatient or outpatient.
- Many patients will not know all of this information when you are asking it the first time and you will need to be mindful to ask in term the patient can understand. For example, patients may not understand peripheral vascular disease, but they may understand they have “ weak pulses” in their feet or “poor circulation”, they may not know what a CVA is, but will understand stroke, etc.
- For family medical history, also understand that many families do not discuss health conditions that are perceived to be controlled. It is not uncommon for patients to tell providers “My X had high BP but she takes medicine and now she is ok”, or “ Her pressure was really bad but now she is on dialysis and doing well”.
Past Medical History: Has the patient ever been told or diagnosed with: congenital heart disease, murmurs, palpitations, abnormal EKG, High blood pressure, MI, high cholesterol, stroke, heart failure, peripheral vascular disease (poor circulation), dialysis, diabetes?
Surgical History: Has the patient ever had a cardiac bypass graft, stent, angioplasty, or pacemaker?
Family Medical History: does the patient know if their mom, dad, siblings or grandparents had any of these conditions? Congenital heart disease, murmurs, palpitations, abnormal EKG, High blood pressure, MI, high cholesterol, stroke, heart failure, peripheral vascular disease (poor circulation), dialysis, diabetes. Did anyone die < age 50 or did anyone die suddenly without a known cause?
Social History: Alcohol, tobacco, other smoking, drugs (list them), other drugs not prescribed for them?
Diet: usual foods, typical day
Occupational: What do they do for work? Any exposures that would be a risk factor for heart disease? (Long distance driver, NFL coach, etc.)
Review of Systems: These systems need to be included in the CV ROS:
- General:
- Skin:
- CV:
- Pulmonary:
- Abdomen:
- Extremities:
Physical Exam
Observation and Inspection:
- Can they walk without taking a break to catch breath or rest legs?
- How do they look sitting in the bed?
- What is their posture like when standing/sitting?
- How quickly do they recover from activity?
- What is their coloring like? Does it change?
- What do their extremities look like?
Palpation:At neck, you look at the arteries and veins
Carotids – palpate and auscultate (thrill & bruit) – ONE SIDE AT A TIME
Jugular veins – indicates right atrial pressure = central venous pressure
Heaves and PMI: Palpate Chest wall, use landmarks
Auscultate Heart Sounds: First use diaphragm (identifies high pitch sounds) for the aortic, pulmonic, tricuspid, and mitral valves then switch to bell (identifies low pitch sounds) and listen to the valves in the opposite order
- “APE TO MAN” or “A Pretty Tough Murmur” are commonly used pneumonics for cardiac landmarks
- Aortic~ R 2nd ICS
- Pulmonary~ L 2nd ICS- base
- Tricuspid~ L 4th ICS
- Mitral~ L 5th ICS, MCL, apex
- Stethoscope positioning
- Bell~ low pitch
- Diaphragm~ high pitch
Normal Heart Sounds:
- S1~ closing of mitral and tricuspid valves (atrioventricular valves)
- S2~ closing of aortic and pulmonic valves (semilunar valves)
- Systole~ S1 occurs at the beginning
- Diastole~ S2 occurs at the beginning of diastole
Abnormal Heart Sounds
Depending upon your practice and patient population you may hear many or none of these abnormal heart sounds routinely. This is a brief synopsis to raise your awareness of heart murmurs. If you hear something that sounds “different”, whether a new or seasoned APRN, it is great practice to ask a colleague to listen to verify what you are hearing.
- S3~Just after S2, apex, left sternal border, bell, low pitch
- Can be innocent or pathologic
- Kids and young adults and pregnant women~ innocent
- Older adults~ pathologic 2/2 HF, Volume Overload, MV or TV regurgitation~ may need to be left lateral position
- Known as ventricular gallop
- S1 S2 S3
- “Sloshing-In”, “Kentucky”
- S4~ Just before S1, supine or lateral, loud pitch
- Can be innocent but usually pathologic
- Can be innocent in well-trained athletes
- Can be pathologic and seen with HTN, CVD, CM, Pulm HTN
- Known as atrial gallop
- S4 S1 S2
- “A Stiff Wall”, “Tennessee”
- Opening snap ~ OPENING of a stenotic (i,.e narrowed) mitral or tricuspid valve
- Left sternal border, early diastole (end of S2), high pitch, diaphragm of the stethoscope
- Pathologic causes include complete heart block, aortic/pulmonic regurgitation
- Friction rubs~ pathologic following an MI or with pericarditis, results 2/2 inflammation of the pericardial sac and the linings rubbing together
- High pitch, grating, scratching sound
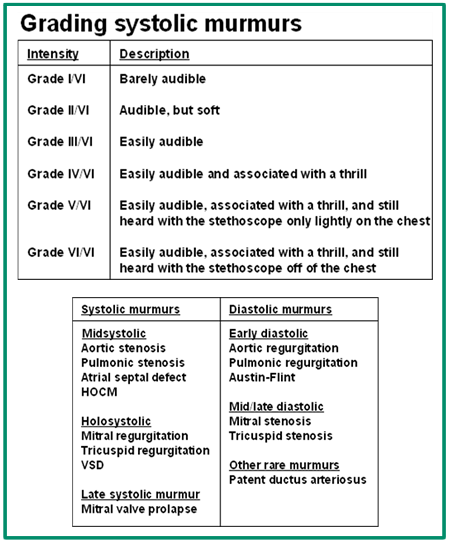
- Murmurs
- Murmurs result from abnormal flow in any direction across the valves. They are either classified as systolic (most common) vs. diastolic (always pathologic). It is helpful to use techniques to amplify murmurs so you can clarify what you are hearing. Some techniques that amplify murmurs include: Stand and Squat, Valsalva, palpate radial pulse while listening.
- Innocent ~ aka physiologic or functional are temporary increase in blood flow, such as anemia, pregnancy or fever. Occur in children and young adults and disappear upon sitting
- Pathologic~ indicates a structural issue, such as aortic insufficiency or VSD
- Click the following links to learn more about heart sounds:
Assessing Jugular Venous Pressure:
Pleae watch: https://www.youtube.com/watch?v=AWxbAg0E3E4
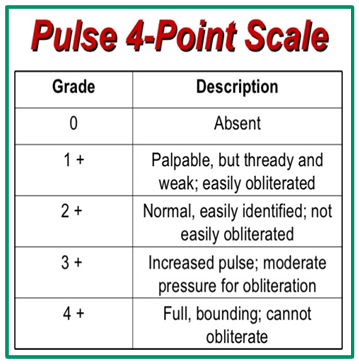
Pulses
Assess pulses at landmarks noted (Ball, page 116). Pulses are documented as 0-4+, most healthy individuals have pulses of 2+.
Assess skin color, temperature, hair distribution as you check the pulses.
This website is maintained by the University of Maryland School of Nursing (UMSON) Office of Learning Technologies. The UMSON logo and all other contents of this website are the sole property of UMSON and may not be used for any purpose without prior written consent. Links to other websites do not constitute or imply an endorsement of those sites, their content, or their products and services. Please send comments, corrections, and link improvements to nrsonline@umaryland.edu.